
Create unlimited WordPress registration forms
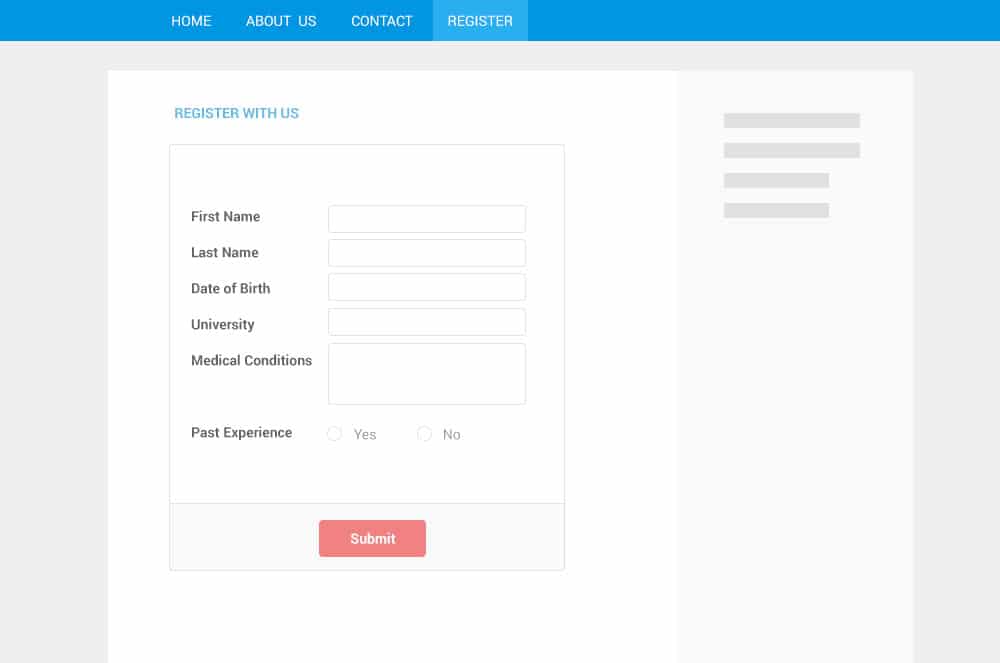
With RegistrationMagic WordPress Registration Plugin, every WordPress registration form is unique. It can have its own set of custom fields, content and configuration. Each WordPress user registration form is represented by a Form Card, which provides at-a-glance view of form submissions, user registrations, shortcuts menu and access to form settings.
幸运168飞艇全国开奖记录历史直播-幸运168飞艇查询结果正规网 -168飞艇在线开奖网站官网 registration form like never before
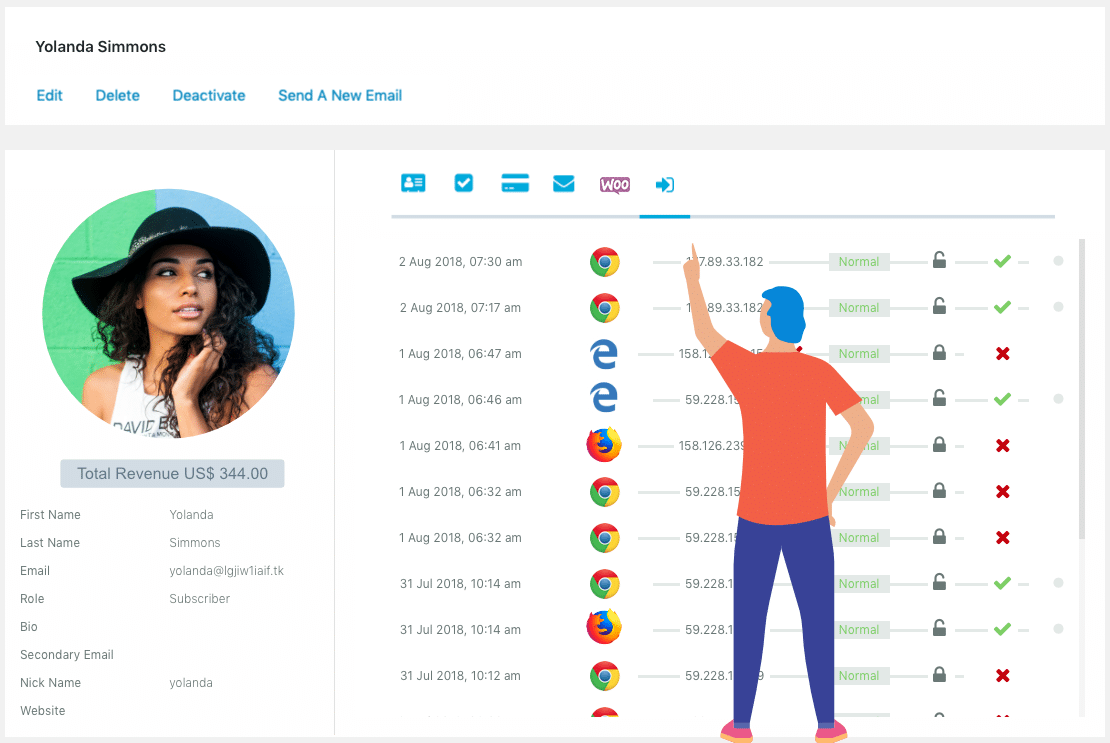
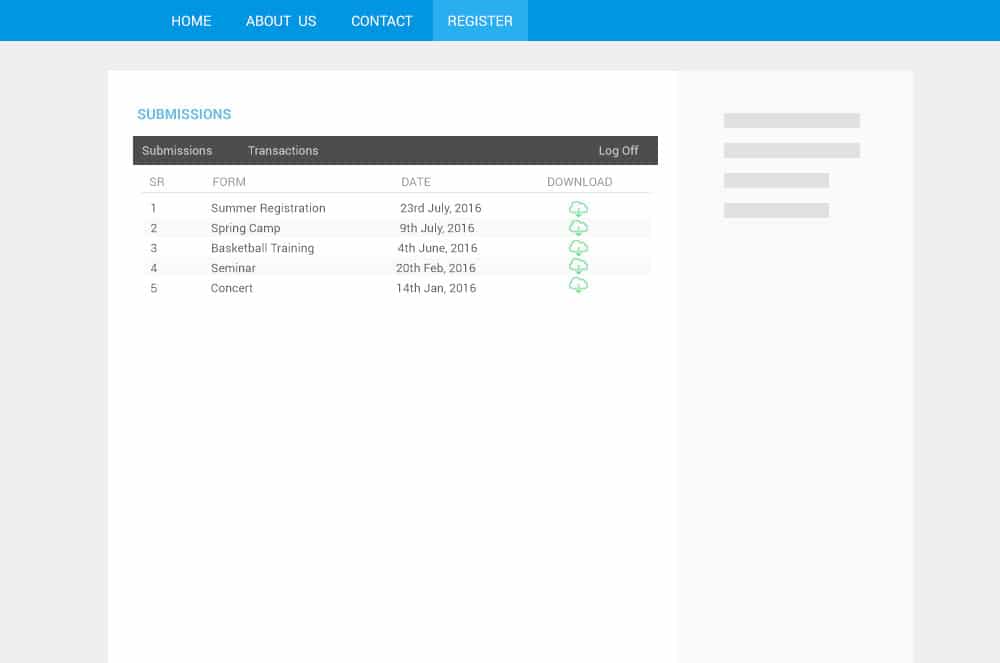
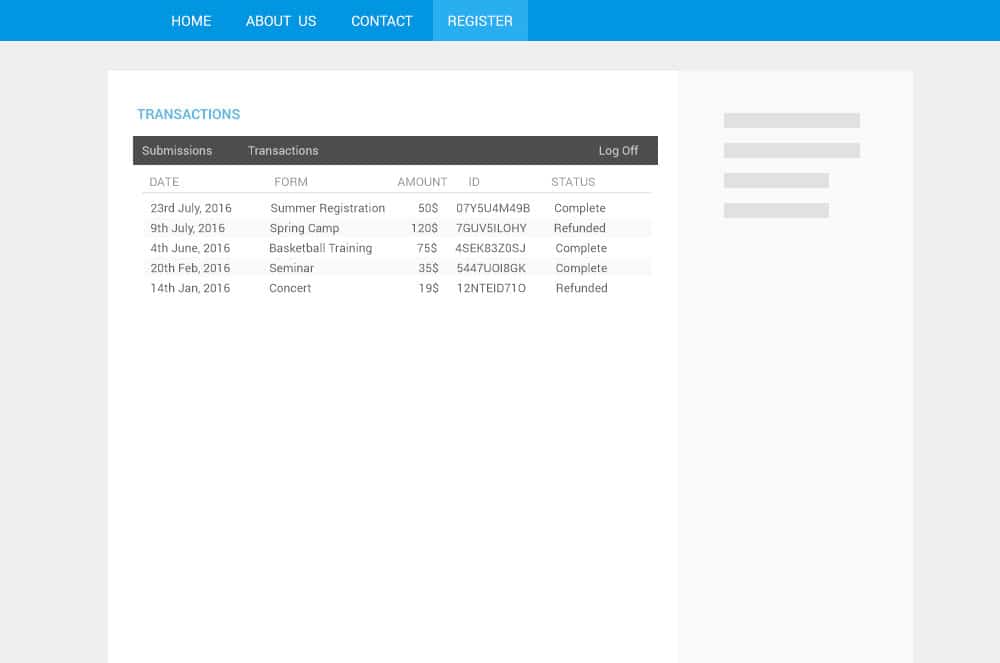
In RegistrationMagic, you can analyze every WordPress user registration form and submission using in-built graphs, charts and tables. This helps you to fine tune your user registration process. You can track user location, IP, browser data and OS, form conversion rate, filling time and a lot more. You can also analyze user login attempts, login timelines, login success vs failure graph, along with other important login parameters. Follow our User Login guide to step-up login analytics and modernize your user login process with two-factor authentication and other advance login features.
Total User Control
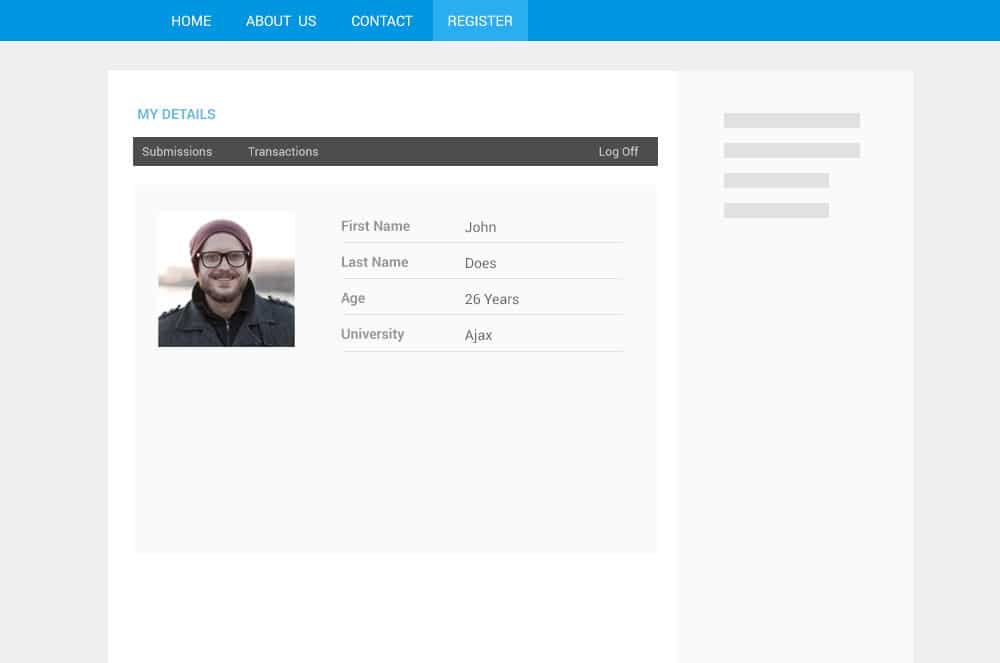
Finally, you can take total control of WordPress user registration on your site. By introducing innovative features like user deactivation and a one time password login system, we have filled in the missing gaps of default WordPress registration system. Not only this, we have introduced (first time ever) custom registration statuses and automation workflows to provide you more control over your post-registration processes too. This is the only WordPress custom registration toolkit you will ever need!



Premium Features
-

I use registration magic to register students for my workshops. I can add all the fields I need, customize the form and the best is I get email notifications when a new student registers. I just use the free version and when I had a small issue with it, the support was right onto it as soon as I requested help. Excellent support. Overall, a wonderful experience with Registration Magic for me.
fabchuckyon WordPress.org -

I loved this plugin! Straightforward, simple, easy, amazing and powerful! Thank you so much!
elisandroborgesOn WordPress.org -

-
This plugin is under active development, there are regular updates. When I had some issues, I had a very good experience with customer support.
romandesign@romandesign on WordPress.org -
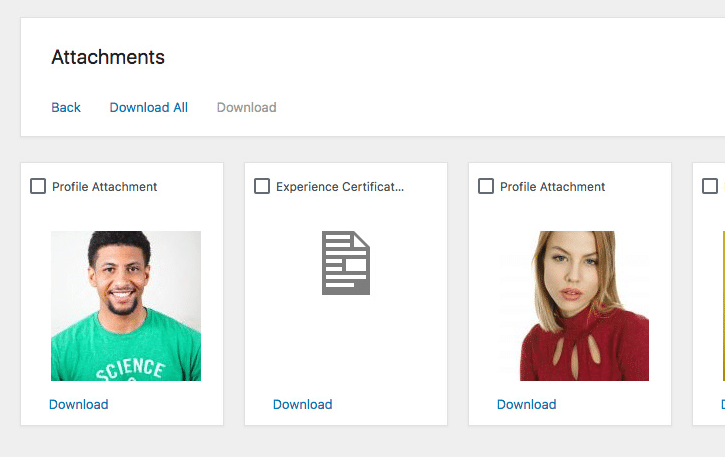
I needed a registration form that could redirect as well as a form to allow multiple file uploads. This plugin gave me all I needed plus more. My site was hacked and messed stuff up but Registration Magic's support was prompt and fixed my issues with no problems. Very knowledgeable, fast and friendly team.
rdpshop@rdpshop on WordPress.org -

That's a best plugin for registration I've ever seen. It works like charm, has optimization, does integrate with template effortlessly, is secure with reCAPTCHA... I needed it to cope with s2memebr and it works great. Great plugin and support is fast, helpful and reliable. Keep doing a great job! 🙂
merlinseducer@merlinseducer on WordPress.org -
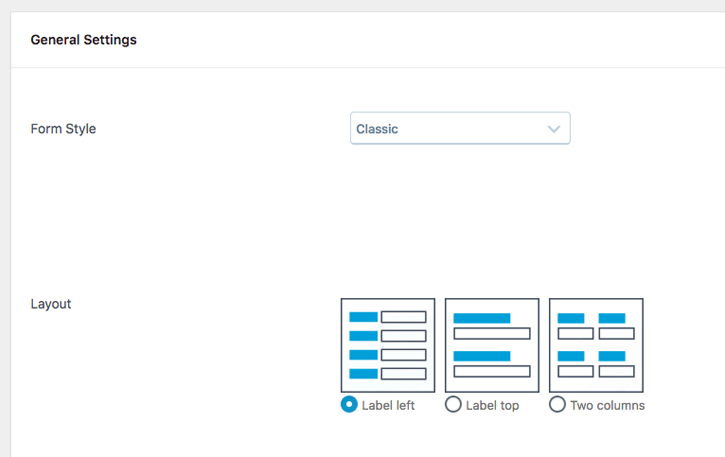
Registrationmagic makes it easy to create forms. You simply choose the type of fields you want to show up, and the form is instantly created.It's really no more complicated than that. No messing with a form layout, or CSS, or shortcodes, except one - the form name. The plugin gives you the shortcode for the form, and you just copy and paste to a page. That's it - you're done. I emailed a concern about a typo I found in a field and Registrationmagic IMMEDIATEly responded and addressed the problem. That kind of prompt service is rare in any business, and much appreciated by me.
stephwalther@stephwalther on WordPress.org -
iAppsWP@iappswp on WordPress.orgI had a number of requirements for an unusual case and after searching for many alternatives that didn't gel, Registration Magic solved a large part of my needs and were even enthusiastic about adding an extra feature that will help my cause even more when implemented. Initially I had some problems with the plugin that appeared to be a bug with the version but support was fantastic. When they were able to get in and take a look, they had it solved even before I'd noticed. Highly recommended. -
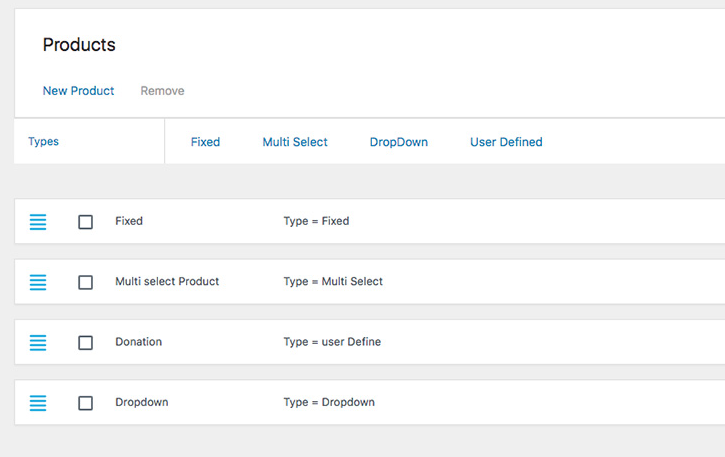
I have started using RegistrationMagic for managing forms on my site and it works just great. The flexibility with number of options it offers are unmatched by any of the other competing plugins. Best of it all is that I never felt intimidated with setting up some of the complex options (such as payments) even though I am not very technical person.
Sarah(@sarahar) on WordPress.org -

This plugin is perfect. Does just as I needed. I am in the process of planning a car show and it has saved me a great amount of work with online registration.
haveyoumetrandy@haveyoumetrandy on WordPress.org